Laparoscopic Living Donor Right Hepatectomy Regarding the Anatomical Variation of the Portal Vein: A Propensity Score–Matched A
Author
jsrrules
Date
2024-12-08 20:29
Views
629

This study is designed to analyze the feasibility of laparoscopic living donor right hemihepatectomy in living donors with portal vein variation. Living donor liver transplantation cases using a right liver graft during the period of January 2014 to September 2019 were included. Computed tomographic angiographies of the donor were 3-dimensionally reconstructed, and the anatomical variation of the portal vein was classified. To reduce selection bias, a 1:1 ratio propensity score–matched
analysis between the laparoscopy group and the open group was performed. Surgical and recovery-related outcomes as well as portal vein complication-free
survival, graft survival, and overall survival rates were analyzed. After matching, 171 cases in each group from 444 original cases were compared. The laparoscopy group had a shorter operation time (P < 0.001), a smaller number of additional opioids required by the donor (P < 0.001), and a shorter hospital stay (P < 0.001). There were no differences in the portal vein complication-free survival (P = 0.16), graft survival (P = 0.26), or overall survival rates (P = 0.53). Although portal vein complication-free
survival was inferior in portal veins other than type I (P = 0.01), the laparoscopy group showed similar portal vein complication-free survival regardless of the anatomical variation of portal vein (P = 0.35 in type I and P = 0.30 in other types). Laparoscopic living donor right hemihepatectomy can be performed as safely as open surgery regardless of the anatomical variation of the portal vein.
Study Focus:
The study evaluates the feasibility and safety of laparoscopic living donor right hepatectomy (LLDRH) in cases with portal vein (PV) anatomical variations, using propensity score (PS)–matched analysis to compare laparoscopic and open surgery approaches.
Key Findings:
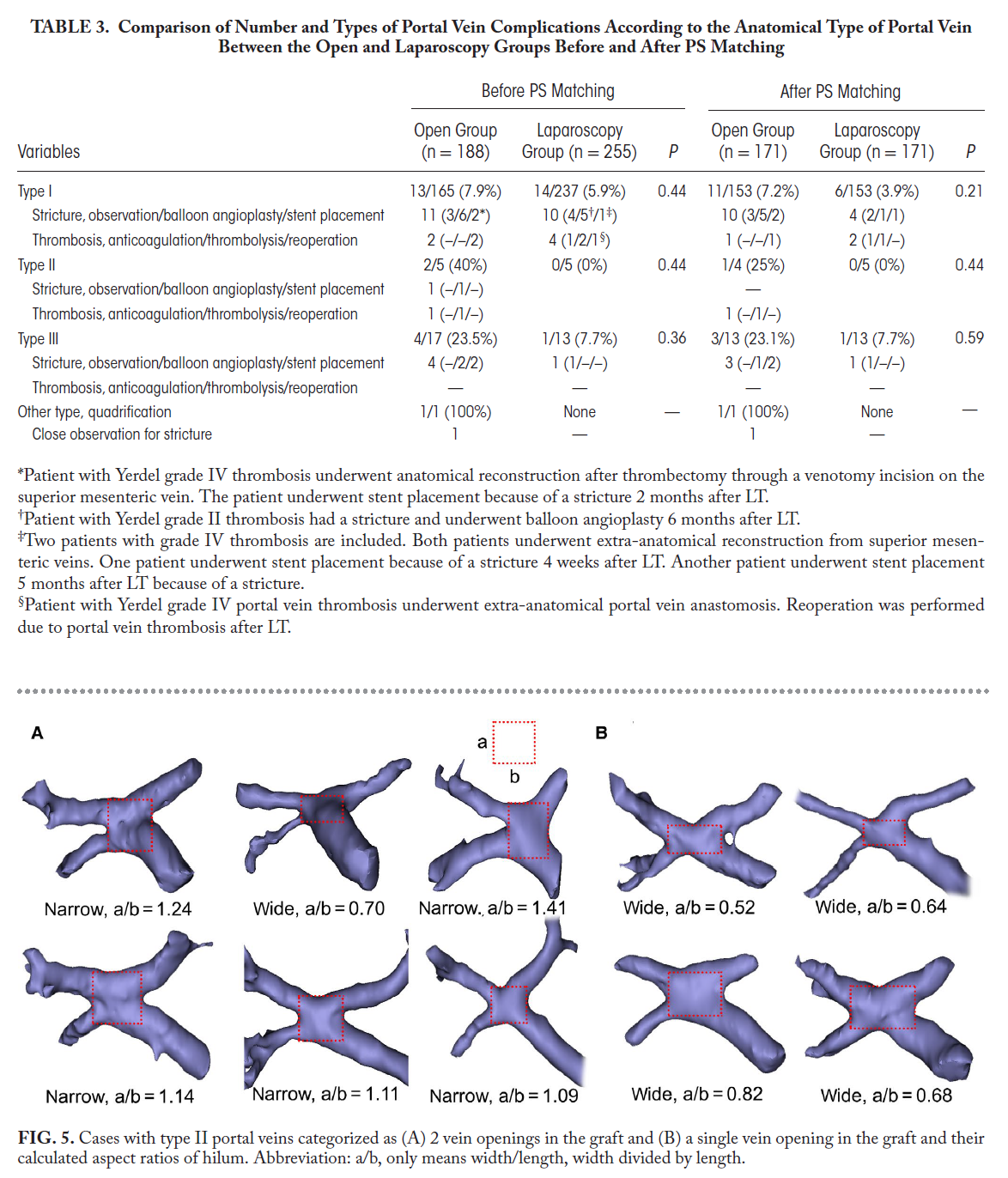
- Portal Vein Variations: PV variations (types II and III) were associated with more grafts having two PV openings, but laparoscopic surgery managed these safely with outcomes comparable to open surgery. Complication rates were similar between laparoscopy and open surgery regardless of PV type.
- Safety and Efficiency: Laparoscopic surgery had shorter operation times, less blood loss, shorter hospital stays, and reduced opioid requirements compared to open surgery. Postoperative PV complication rates requiring intervention were lower in the laparoscopy group (1.8% vs. 7.0%, P = 0.03).
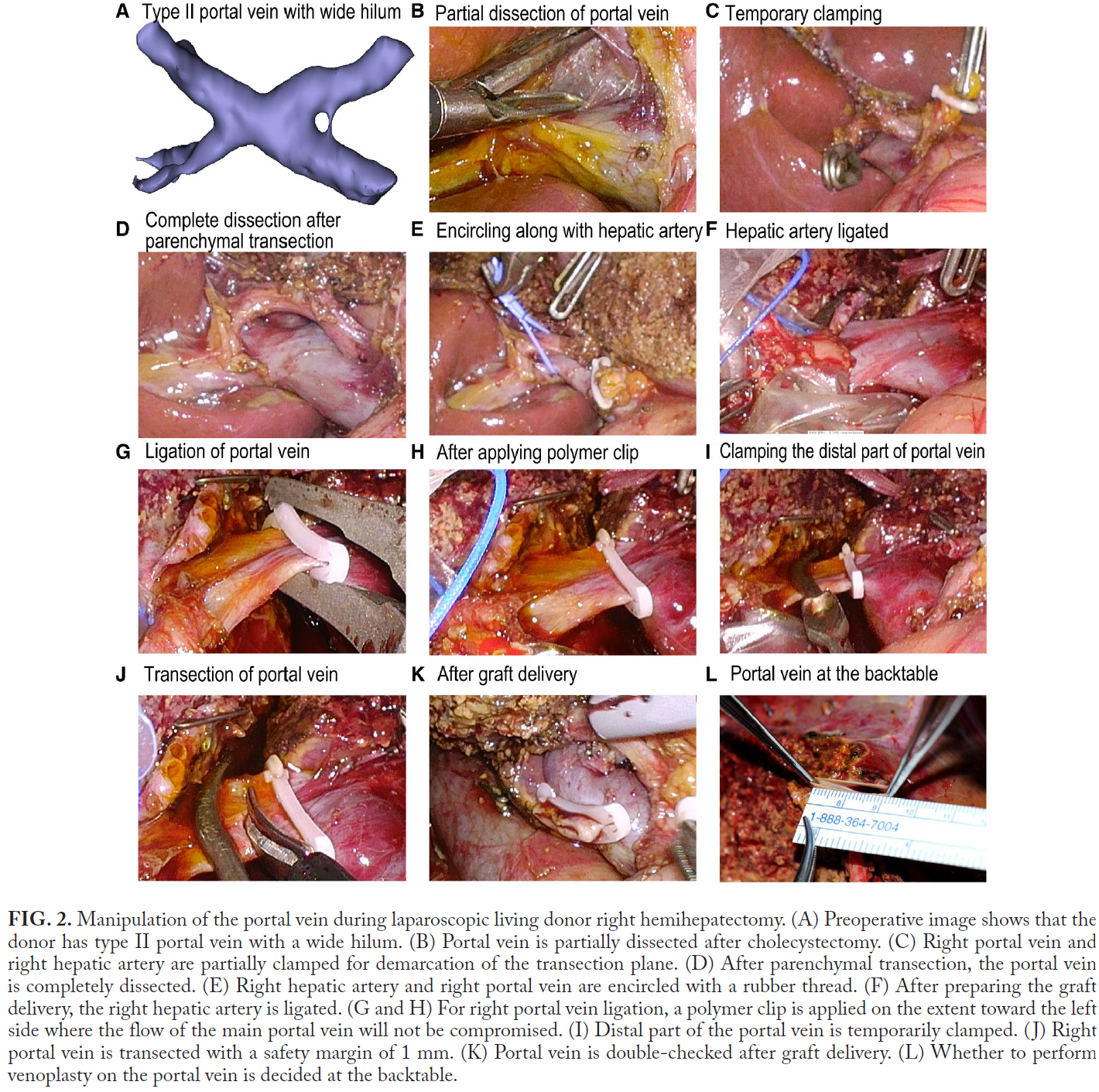
- 3D Modeling: Preoperative 3D reconstructions of donor PV anatomy aided in surgical planning, especially for complex PV types, improving precision and safety.
Conclusion:
LLDRH is a safe and effective alternative to open surgery, even in cases with challenging PV variations, provided the surgical team has sufficient expertise.
3D modeling in laparoscopic liver surgery is pivotal for visualizing complex PV anatomy, improving preoperative planning, and enhancing surgical safety and precision. By reducing complications and streamlining procedures, 3D modeling facilitates the broader adoption of minimally invasive techniques in liver transplantation.
연구 초점:
이 연구는 문맥(portal vein, PV) 해부학적 변이를 가진 생체 공여자 간 우엽 절제술에서 복강경 수술의 안전성과 타당성을 평가하기 위해 성향 점수(PS) 매칭 분석을 사용하여 복강경 수술과 개복 수술을 비교했습니다.
주요 결과:
- 문맥 변이: PV 변이(II형 및 III형)는 두 개의 문맥 개구부를 가지는 경우가 더 많았지만, 복강경 수술에서도 안전하게 관리되어 개복 수술과 유사한 결과를 보였습니다.
PV 변이 유형에 관계없이 복강경과 개복 수술 간 합병증 비율은 유사했습니다.
- 안전성과 효율성: 복강경 수술은 개복 수술에 비해 수술 시간 단축, 출혈량 감소, 입원 기간 단축, 진통제 요구량 감소 등의 장점을 보였습니다. 수술 후 문맥 합병증 발생률은 복강경 그룹에서 더 낮았습니다(1.8% vs. 7.0%, P = 0.03).
- 3D 모델링: 공여자의 PV 해부학적 구조를 3D 재구성하여 복잡한 PV 유형에서도 수술 계획을 개선하고 정밀도와 안전성을 높였습니다.
결론: 충분한 경험을 가진 외과 팀이 수행한다면, 복강경 생체 공여자 간 우엽 절제술은 어려운 PV 변이를 가진 경우에도 안전하고 효과적인 대안으로 자리 잡을 수 있습니다.
복강경 간 수술에서 3D 모델링은 복잡한 문맥 해부학을 시각화하고, 수술 전 계획을 개선하며, 수술 안전성과 정밀성을 높이는 데 중요한 역할을 합니다. 합병증을 줄이고 절차를 간소화함으로써, 3D 모델링은 간 이식에서 최소 침습 기술의 광범위한 채택을 촉진합니다.
📥 다운로드 횟수: 50회